As any regular reader of this site is aware, I have been very vocal about the various changes to Medicare proposed by the LNP government. A list of past articles is provided at the end of this article should you have missed out. I also appeared on the ABC News supporting the RACGP in their “You’ve Been Targeted” campaign.
Earlier this week I wondered what was happening. Minister Ley had promised to consult with doctors before making any changes. I’d suggested Ley not forget about the most important demographic: the patients. I Googled and didn’t find much. I checked Ley’s Twitter feed and found the odd tweet about consulting with doctors.
https://twitter.com/MalBrough_MP/status/563504992078688257
Meeting with doctors and
more doctors.
Where are the meetings with PATIENTS? This one, maybe?
Possibly, but they look suspiciously like more medicos to me. I was becoming a little depressed. Yesterday Ley finally held a press conference. The full transcript is available: Update on nationwide Medicare policy consultation.
Craig Laundy: It’s great to have the Health Minister, the Honorable Sussan Ley and my good friend the Member for Lyne Dr David Gillespie here in Reid for an afternoon of consulting with local GPs so without further ado Sussan welcome.
Not one word about PATIENTS! More doctors! Yes, doctors are voters, just like you or I. Yes, doctors pay the Medicare levy just like you or I. Yes, doctors have a vital voice in any changes to Medicare. You and I have a far greater voice and we must not let Ley forget that.
I’ve just come from breakfast this morning on the Central Coast. There were 40 doctors and lots of different views in the room and the same for last night and I’m on my way to another part of the country to do something similar.
Still no mention of PATIENTS. *sigh*
…accept that unless you’re in a vulnerable category maybe those services don’t come absolutely for free and that where there is an ability to pay that you value the high quality service that you receive that you do indeed pay something. When I look at the number of bulk-billed consultations across the country 76 per cent of all episodes of care are bulk-billed to non-concessional patients.
No, Ley, any bulk-billed service to a non-concessional patient is certainly not for “absolutely free” as most non-concessional patients are working and paying the Medicare Levy! Or are the children of people paying the Medicare Levy. That’s not “free”, we pay an insurance premium. I’ve heard it said there are medical practices that bulk-bill 100% of their consultations. I’ve yet to actually attend one, but I have no doubt there are some. There are also practices that bulk-bill only those holding a Health Care Card.
The practice I go to has a policy of bulk-billing walk-ins (see first available doctor) between 7 am and 6 pm. Appointments are not bulk-billed, nor are consultations after 6 pm or on weekends or public holidays. I think there are many practices with similar policies. How often am I a walk-in? Not too often. I work full-time and also have medical conditions which I prefer to have overseen by a regular doctor. Consequently most of my consultations are either by appointment or outside of the bulk-bill hours, even if I am walking in with a child that needs a stitch in a toe – no appointment, but 8 pm at night. $90 payment, $49 rebate. My co-payment is already $41, thank you very much. The average patient contribution for out-of-hospital services for patients who pay is $51 (including specialists visits).
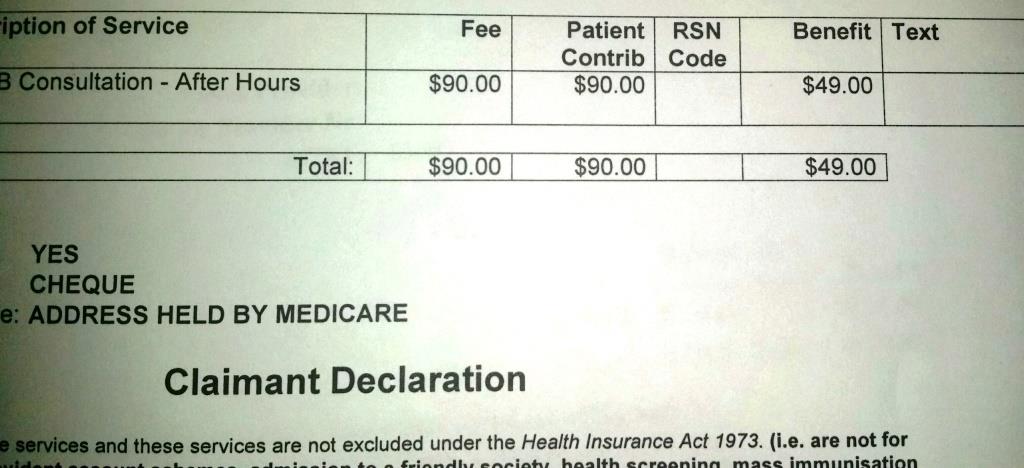
My GP visit
I wanted to see proof of this 76%. I thought the annual report might be a good place to start, but as Medicare has been absorbed into the Department of Human Services, there doesn’t seem to be much Medicare detail in that report. The Department of Human Services ended the 2013-14 year with an operating SURPLUS.
In 2013–14 the department administered an estimated $159.2 billion in payments or around 38 per cent of government outlays. Financial performance targets were met, for the most part, and the department reported an operating surplus of $132.6 million after adjustment for unfunded depreciation and the revaluation of assets. This compares with a deficit of $7.7 million in 2012–13.
That doesn’t tell me anything about bulk-billing though, interesting as the information may be. Further research found bulk-billing statistics. Click the image to go to the full table. According to the Medicare statistics, 77.2% of consultations were bulk-billed for the 2013-14 year, but there are vast differences across services. GP visits are bulk-billed 82.2% of the time, whereas specialists a mere 29.2%. No clear differentiation is given in the report between concessional and non-concessional patients, so are we to assume only 1.2% of consultations were for concessional patients?
Clearly doctors in Canberra don’t believe in bulk-billing politicians.

I am struggling to believe the rate is this high. If you want to delve into the full statistics yourself, the spreadsheet available is very useful.
Why is the rate of bulk-billing so high? Based on my own personal experience and that of friends, family and co-workers, my guess would have been less than 50%. The history of Medicare may have something to do with it. I found this interesting snippet. Read very carefully.
Levels of bulk billing for unreferred GP attendances have been declining in recent years after reaching a high of 79.7 per cent in1996-97. By the December quarter 2002 bulk billing for unreferred GP attendances had declined to 68.8 per cent, but by June 2004 this had improved to 70.2 percent.
Source: APH
The decline in bulk-billing had been viewed as a negative! Incentives of $7.50 to encourage doctors to bulk-bill were introduced in 2004.
From 1 May a $7.50 incentive paid to GPs for bulk-billed GP consultations with concession card holders and children under 16 in non-metropolitan areas (RRMAs 3-7) and Tasmania introduced. This incentive replaces the earlier $5 incentive in these areas.
As of 1 September eligibility for the $7.50 incentive payment to GPs extended to eligible urban areas and large regional centres.
Clearly bulk-billing was encouraged in more ways than one.
Between 1992 and 2003 the Scheduled Fee rose 26%. The CPI rose 31%. Doctors were taking a pay cut.
Interestingly, during the 2004 election campaign, the Coalition proposed to increase the rebate to 100% of the scheduled fee. Different captain at the same helm eleven (eleventy?) years later wants to cut the rebate.
Proposals for changes to Medicare were announced by the Coalition during the 2004 election campaign. These include from 1 January 2005 increasing the Medicare rebate for all GP services to 100 per cent of the Schedule fee…
Source: APH Library Archive
When did the big clinics emerge? Edelsten opened the first after Medicare came into being in 1984. We now have very professional corporate medical businesses, minus the chandeliers and gawdy trimmings.
Reading through the history, it is clear Medicare has been tweaked many times over the years. The practice of medicine has evolved. We no longer visit our local family doctor in the front room of his residence as in days gone by. The economies of scale from multi-disciplinary and multi-doctor practices would, I think, be necessary in circumstances where fee increases were running well behind CPI increases AND bulk-billing was being encouraged.
The HICAPS system has been a great innovation. The doctor gets paid at the time of service and the patient receives the rebate overnight in their bank account. As noted in the past, I’ve actually received the rebate credit before the payment debit hit my bank account. For patients this saves considerable time. In the last twelve months I’ve only visited one medical provider (and we know I’ve visited a few) that had not yet moved to HICAPS. Gone are the days of lining up in a Medicare office to claim medical bills.
The medical profession was initially resistant to Medicare. The medical profession today is a very different beast to the medical profession of forty years ago. Many practitioners are not as politically right wing as their predecessors. Free university education saw many from different backgrounds obtain degrees.
Forty years is a long time. You may be reading this on a smartphone. Medicare was launched three years before Telstra launched the first mass mobile network in Australia. The phone cost $5,200. Technology, medicine, society: all have changed.
How much revenue does the Medicare Levy raise? That seems to be the greatest secret, as despite considerable research, I can’t find the answer. The spreadsheet I referred to above analyses the costs of Medicare to the nth degree, sliced and diced to within an inch of the core and tells me the benefits paid were $19.1 billion. Not a revenue number in sight. Nor, for that matter the infrastructure, staff and other costs (such as HICAPS).
Was Medicare ever intended to be completely self-funding?
The objectives of the original Medibank were summarised by R. B. Scotton (1977) as universal in coverage, equitable in distribution of costs, and administratively simple to manage.
That statement doesn’t really specify self-funding. As it turns out, the original funding bills weren’t passed and the funding came from general revenue. The levy came later.
“Equitable in distribution of costs” doesn’t mean the same thing as self-funding. In any case, what was appropriate forty years ago may not be appropriate today – and that could be either way. How do we assess “equitable”? These are social questions, not medical questions, yet I see Ley focussing on the medical profession and not the people.
Continued: Medicare is not the problem
Previous Medicare related articles:
- How much does it cost to COMPLETELY collect and process that $7?
- You’ve been targeted: supporting the AMA and RACGP supporting us
- How Medicare Rebate cuts may impact the patient, other than cost
- In the Australia of the future, you will fly out to see a doctor
- Medicare is YOUR insurance cover
- What is this premature performance costing the taxpayer?
- Open Letter to Sussan Ley on Medicare changes
- The growth of Medicare is slowing


[…] This article continues from Sussan Ley updates the nation on Medicare. […]
LikeLike
I don’t know of any doctors that don’t bulk bill in my area. I would say it would be 100%. Even pathology and radiology, psychology are bulk billed. This is a low socioeconomic area with a lot of migrants, families with young kids, low income earners and pensioners. If people around here had to pay a co payment a lot of them would go to local hospital or not go to the doctor at all. So I think rates of bulk billing vary greatly from area to area.
LikeLiked by 2 people
Susan, I’ve approved both comments because they are slightly different and your point here about going to hospitals is very important to the discussion.
LikeLiked by 2 people
Oops! I only meant to leave one comment but I had to reset my wordpress password and I thought my first one had disappeared so I wrote another one!
LikeLike
I figured it was something along those lines, but the additional thought was very valid! 🙂
LikeLike
not sure if this is what you were after
“revenue from the Medicare levy—a 1.5% levy on taxable income—is estimated to total $10.3 billion in 2013–14, but is forecast to grow by nearly 60% to $16.2 billion in 2016–17…”
http://www.aph.gov.au/About_Parliament/Parliamentary_Departments/Parliamentary_Library/FlagPost/2014/February/How-much-Medicare-cost
LikeLiked by 1 person
Thanks Helena! Very useful! I knew it had to be available SOMEWHERE, but was like trying to find a needle in a haystack!
LikeLike
There are very few practices that don’t fully bulk bill in my area, in fact I don’t know of any. Even pathology, radiology and some specialists bulk bill. It’s a low socio economic area with a lot of pensioners and parents with young kids. I would think bulk billing is pretty close to 100% around here.
LikeLiked by 1 person
Definitely agree there were would be socio-economic considerations, Susan. There will be areas where it would be close to 100%, I have no doubt. Youth unemployment is particularly high currently and that will also impact. The student population, children – but are children really “non-concessional” if there is an incentive to bulk-bill children and their parents are not concessional?
LikeLike
Thanks for pulling all the information,or what is available,together Robyn.Often difficult to make informed decisions about the rhetoric politicians engage in when there is so much uncertainty about the facts in the first place! I too am concerned about the lack of consultation with patients. I am one of those people who can afford to pay the current “co-payment” or indeed a further introduced “co-payment” but that is not the point,I am concerned that the issue is a political one not an economic one!
LikeLiked by 1 person
I do think there are economic considerations, but it is definitely a social consideration primarily in my view. What sort of a nation do we want? The USA? I suggest not. I believe the vast majority of Australians want universal medicine and universal education. Once we have decided that, then we move on to considering the economic considerations: how do we pay for it? For it does have to be paid for – everything has to be paid for one way or another, ultimately.
We are one of the most highly taxed countries in the world, partly because we have a small population and like our services – so we need to find, dare I say it, equitable solutions!
LikeLiked by 1 person
True! There is an economic issue with all of our services as you say! If we want services we have to pay for them somehow!However, by not returning the “copayment” to Medicare the govt shows that the financing if Medicare is not their prime consideration and going on their track record appears just another attempt at dismantling anything Labor has achieved over the years. There are many other options to raise revenue that they simply ignore based on ideology not good policy! But that’s what governments are about.We pay taxes, govt prioritises how those taxes are spent. This is why we depend on access to information so we can evaluate whether those priorities will benefit the community as a whole or will it disadvantage some groups in favour of others! In my opinion this would be first step in privatising all medical services & we would end up like America where you have to be rich to get good care…we were heading that way in the 60s and we know how Whitlam & then Hawke prioritised health as a universal right.
Thank you being a strong voice in the debate as MSM is not doing its job very well to keep people informed or giving them a voice to express the opinions the govt seems to not want to listen to!
LikeLiked by 1 person
Excellent piece Robyn. You’ve hit the mark again. This government has a particularly neo-con perspective on consultation, and on recipients of services funded by government. Looking forward to your next instalment.
LikeLiked by 2 people
Thank you Michaela. Too much for one article! This has to be by instalments.
At this rate, I may be able to publish a book on Medicare from the articles! 🙂
LikeLiked by 3 people